Bile duct cancer (Cholangiocarcinoma)


Bile duct
The bile duct is a network of thin tubes, which collects bile from the liver and drains it into the intestine. Bile is a fluid made by the liver to aid digestion of fats in the intestine.
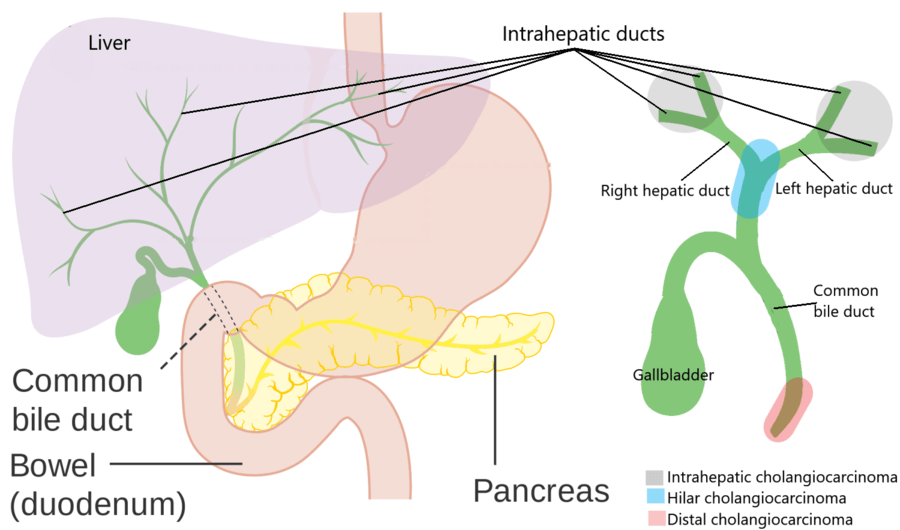
The bile duct is a tree-like structure with multiple branches in the liver, which then combines to form right and left hepatic duct draining right and left lobe of the liver. These two then join, the joint called hilum or confluence, becomes the common bile duct (gallbladder also connects to it through cystic duct). Common bile duct then continues downstream, is joined by pancreatic duct and opens into the intestine (in the part of the intestine called the duodenum).
Bile duct cancer is also called cholangiocarcinoma. In this cancerous cells form in the bile duct and then grows and spreads.
Bile duct cancer (cholangiocarcinoma) is of three types, depending on the part of the bile duct it arises from.
Types of bile duct cancer
Intrahepatic bile duct cancer (cholangiocarcinoma): The bile ducts located within the liver are intrahepatic. In intrahepatic cholangiocarcinoma, cancer originates in these ducts. Read more about it here.
Perihilar bile duct cancer (cholangiocarcinoma): This term describes cancer arising from the bile duct at the hilum or confluence (remember, this is where right and left hepatic duct joins to form a single tube). It is also called hilar cholangiocarcinoma or Klatskin tumour. Read more about it here.
Distal bile duct cancer (cholangiocarcinoma): This occurs in the part of the bile duct which is close to its entry into the intestine, where it passes through the head of the pancreas. Read more about it here.
Perihilar and distal bile duct cancer are together termed extrahepatic (outside the liver) bile duct cancer.
Risk factor or causes of bile duct cancer
Anything that increases your chance of getting a disease is called a risk factor. A risk factor does not necessarily cause the disease, it just increases the probability of getting the disease.
Risk factors for cholangiocarcinoma include:
- Primary sclerosing cholangitis (a disease in which the bile ducts progressively become scarred and then get blocked)
- Ulcerative colitis and Crohn disease (Inflammation of the large intestine)
- Cysts of the bile duct (choledochal cyst)
- Infection with a parasite called the liver fluke
- Cirrhosis and Viral hepatitis (hepatitis B and C)
- Hepatolithiasis (stones in the liver) and choledocholithiasis (stones in the bile duct)
- Toxins e.g. thorotrast
- Smoking and alcohol abuse
- Diabetes and obesity
Signs and symptoms of bile duct cancer
Signs and symptoms are how our bodies indicate that something is wrong. Signs and symptoms of bile duct cancer depend on its type.
Symptoms of cholangiocarcinoma include:
- Jaundice (yellowing of the eyes, urine and skin)
- Abdominal pain
- Fever
- Itching
- Weight loss and loss of appetite
Diagnosis and staging of bile duct cancer
Once a diagnosis of bile duct cancer is suspected based on the clinical features, tests are done to diagnose and stage the disease. The exact tests depend on the type of cholangiocarcinoma we are dealing with, but generally includes:
Blood tests
These include routine blood tests and liver function test.
Tumour markers
These are substances whose level in blood may rise in the presence of specific cancers. In bile duct cancer CA 19-9 and carcinoembryonic antigen (CEA) may be increased.
Ultrasound
This is a basic test to see the liver and bile ducts.
Computed tomographic scan (CT)
Thin cut triple-phase CT is done to visualise cancer and the involved parts of the organs.
Magnetic resonance imaging (MRI) and magnetic resonance cholangiopancreatography (MRCP)
MRI uses strong magnetic fields, radio waves and computer to generate images of inside organs. This imaging modality gives a detailed view of the bile duct and cancer.
Positron emission tomography (PET)
It is a functional imaging technique which is sometimes used for staging.
Biopsy or cytology
In this procedure, a small sample of tumour or few cells from this is obtained and examined under the microscope confirming the diagnosis. This is usually not required in bile duct cancers which can be removed surgically.
Treatment of bile duct cancer
Detection at a stage where they can be removed by surgery, offers the best chance of cure. The surgical option depends on the type of cholangiocarcinoma.
Surgery for bile duct cancer
For intrahepatic and perihilar cholangiocarcinoma, the surgery entails some form of liver resection, also called hepatectomy. The surgical procedure to resect distal cholangiocarcinoma is a Whipple procedure or pancreaticoduodenectomy.
Many times the level of jaundice is too high for upfront surgery and in such cases, jaundice needs to be decreased before surgery by draining the bile. The procedure to drain bile is called Endoscopic retrograde cholangiopancreatography (ERCP) or Percutaneous transhepatic biliary drainage (PTBD). These drainage procedures are also needed in surgically unresectable cases as a means of palliation.
Treatment of advanced bile duct cancer
Tumours which cannot be removed surgically are treated by chemotherapy and/or radiotherapy. Chemotherapy is the use of special drugs to kill cancer cells and radiotherapy is the use of high-powered X-ray beams to kill cancer cells.
To read more about each type of bile duct cancer, follow the respective link:
- Intrahepatic bile duct cancer (cholangiocarcinoma)
- Perihilar bile duct cancer (cholangiocarcinoma)
- Distal bile duct cancer (cholangiocarcinoma)
Detect Early, Treat Right, Save Lives!

About Author
Dr. Nikhil Agrawal
MS, MCh
Dr. Nikhil Agrawal is a leading GI-HPB Surgical Oncologist with 20+ years of experience in complex cancers of the esophagus, stomach, colon, rectum, liver, pancreas, gallbladder, and bile ducts. He leads the GI-HPB Oncology Program at Apollo Hospitals, Delhi and Gurugram, with expertise in advanced robotic and laparoscopic cancer surgery.
His practice focuses on evidence-based, multidisciplinary care with an emphasis on individualized treatment and long-term outcomes.
He trained at BHU, SGPGI Lucknow, AIIMS New Delhi, and SNUBH, South Korea, and is a robotic surgery proctor who trains surgeons in advanced GI-HPB cancer surgery. He is also regularly invited as faculty at national and international scientific meetings.
This website helps patients and families understand GI and HPB diseases and cancers, treatment options, and what to expect during recovery and long-term care.