Colon Cancer



Overview
Our gastrointestinal system digests food and absorbs nutrients. Oesophagus, stomach, small intestine and large intestine makes up the digestive system. The large intestine starts with the colon, which is about 5 feet long and ends in the rectum and anal canal. Caecum and ascending colon, transverse colon, descending colon and sigmoid colon are four parts of the colon.
The colonic wall has four layers of tissue. Cancer occurs when cells in the body grow uncontrolled. Colon cancer begins in the innermost layer, the mucus-producing cells that line the colon.
Most colorectal cancers start as small mounds of flesh called polyps.
Over time, some of these polyps develop into colon cancer. It then advances through the colonic wall and to the adjacent lymph nodes and spreads across the body.
Not all polyps develop into cancer. The chance of a polyp developing into cancer depends on the type, size and number of polyps.
Broadly there are two types of polyps:
- Adenomatous polyp (adenomas): These can develop into cancer.
- Hyperplastic and inflammatory polyps: More common and do not develop into cancer.
Colon cancer is highly curable if detected early and treated appropriately.
Colon cancer and rectal cancer share biology and are discussed together as colorectal cancer. Most of these cancers are adenocarcinomas. Rarely, neuroendocrine (carcinoid) tumour, gastrointestinal stromal tumour, lymphoma and sarcoma can also occur in the colon.
Few facts about colorectal cancer:
Cause and risk factors for colon cancer
DNA of a healthy cell sometimes develops a mutation during cell division. This leads to uncontrolled growth forming a tumour.
Anything that increases the risk of someone getting cancer is a risk factor. The risk factor does not directly cause the disease.
Some with many risk factors will not have the disease, while some with no known risk factor will get it.
Risk factors for colon cancer are:
- Older age
- Western diet (a diet rich in fat, red meat and processed meat; low fibre diet)
- History of colorectal polyps (adenomatous polyp, large polyps and multiple polyps)
- Family history of colorectal cancer (1 in 3 people who develop colorectal cancer have family members who had it)
- Previous history of colorectal cancer (if you have been treated for colorectal cancer earlier)
- Inflammatory bowel disease of the colon; ulcerative colitis and Crohn's disease (the risk of cancer increases with duration and severity).
- Diabetes
- Obesity
- Physical inactivity
- Smoking and alcoholism
Genetic Risk factors (inherited syndromes)
A small percentage of patients, (about 5%) who get colorectal cancer have gene mutations which run in families and increase the risk.
The most common inherited colon cancer syndromes are:
Hereditary nonpolyposis colorectal cancer (HNPCC): HNPCC, also called Lynch syndrome, increases the risk of colon cancer and some other cancers. People with HNPCC develop colorectal cancer before age 50.
Familial adenomatous polyposis (FAP): FAP is a rare disorder that causes you to develop thousands of polyps in the lining of your colon and rectum. People with untreated FAP have an increased risk of developing colorectal cancer before age 40.
Other rare inherited syndromes:
- Peutz-Jeghers syndrome
- MYH-associated polyposis
Symptoms of colon cancer
Colorectal cancer like most gastrointestinal cancers is asymptomatic in initial stages.
The symptoms if occur, include:
- Change in bowel habits; persistent diarrhoea, constipation or the feeling that the bowel does not empty completely
- Unexplained fatigue and loss of appetite
- Unintentional weight loss
- Fall in haemoglobin (anaemia)
- Pain or discomfort in the abdomen
- Patches of bright red or black blood in the stool
Note that many of these symptoms can occur in diseases other than colorectal cancer.
Diagnosis of colon and rectal cancer
Physical history and examination
Understanding symptoms and checking for signs by a physician are basics of arriving at a diagnosis.
Faecal occult blood test (FOBT)
Tumours lose tiny amounts of blood, even when they do not visibly bleed. It can be detected by these tests.
They are of two types:
- Guaiac FOBT
- Faecal immunochemical test \u2013 a newer and better test.
Colonoscopy
Colonoscopy establishes the diagnosis of colorectal cancer.
The colonoscope is a flexible thin tube with a camera. It transmits images from inside of your colon to a monitor. If any abnormality is present, then a small sample from it is obtained, called biopsy. Before the colonoscopy, bowel preparation is done to clean the colon.
Virtual colonoscopy
A specially done CT scan to examine the colon. It is also called colonography or CT colonography.
Biopsy
Biopsy means sampling a small part of the tumour and examining it under a microscope, this is done by a pathologist. Gene tests can also be done on biopsy samples if required.
Determining the extent of colon cancer (staging)
The cancer cells break away from the primary tumour and spread through the body in one of the three ways:
- Bloodstream
- Lymphatic system
- Directly through the tissue

The spread could be; local, through the layers of the colon, to the adjacent lymph nodes and the nearby organs. Or, the spread could be distant, to the liver, lungs and the peritoneum. The distant spread is metastasis.
Staging is finding out the extent of disease. After the diagnosis of colon cancer, we do tests to find out how much the tumour has spread.
Depending upon the suspected extent, we do few of the following investigations to determine the exact stage:
Blood tests: Complete blood count measures the distinct types of cells in the blood. Some patients have anaemia (low haemoglobin). Besides, liver and kidney function tests assess the function of these organs.
Tumour markers: Most colon cancers produce a substance called CEA (carcinoembryonic antigen). A blood test checks its level in the blood. It is a useful test to monitor for recurrence after treatment.
Computed tomography (CT) scan: In this, the patient is placed in a scanner and beams of X-rays image the inside of the abdomen from all sides. These images are then computer-processed giving an accurate representation. Contrast injected into the blood enhances these images.
Magnetic resonance imaging: Instead of x-rays it uses radio waves, and strong magnetic fields.
Positron emission tomography (PET) scan: Cancer cells take up a larger amount of glucose. Here, injected radioactive glucose (18F-fluorodeoxyglucose; FDG) binds to the tumour, and then the patient is imaged. The images are computer-processed and combined with CT images, giving us a CT image with bright tumours.
This work-up will help us assign a stage to the tumour, broadly classifying them into:
TNM (Tumour, Node and Metastasis) classification
Developed by the American Joint Committee on Cancer (AJCC), used for exact classification of the stage. It is based on the following three key elements and span from I to IV.
The extent (size) of the tumour (T): How far has cancer grown into the layers of the colonic wall? Has cancer reached nearby structures or organs?
The spread to nearby lymph nodes (N): Has cancer spread to nearby lymph nodes? And to how many?
The spread (metastasis) to distant sites (M): Has cancer spread to distant lymph nodes or distant organs such as the liver or lungs?
Numbers and letters after T, N and M give further details. Higher the number, more advanced the tumour. Combined Information from T, N and M assigns an overall stage, a process called stage grouping. Colorectal cancer stage ranges from I to IV.
Stages I to III are localized disease and stage IV is advanced cancer (metastatic disease).
Chances of recovery from cancer (prognosis) depend on the stage of the disease at the time of diagnosis. Lower the stage, better is the long-term prognosis.
The definite stage is determined after surgery by histopathological examination of the removed cancer specimen. It is called surgical staging. The stage determined after imaging tests is the clinical stage.
Treatment of colon cancer
The treatment of colon cancer depends on the stage and location of the tumour.
Treatment of localized disease - surgery
Surgery is the primary treatment for earlier stage colon cancer.
Surgery for colon cancer - Colectomy
Partial colectomy, hemicolectomy or segmental resection
It entails the removal of the diseased colon with a margin of healthy tissue and adjacent lymph nodes. Intestinal continuity is then re-established by joining the ends of the intestine (anastomosis). This surgical procedure broadly called partial colectomy has various names depending on the segment of colon resected; right hemicolectomy, left hemicolectomy, sigmoidectomy, transverse colectomy, extended right or left hemicolectomy and anterior resection.
Occasionally, when the tissues are not healthy, the anastomosis is unlikely to heal. In such cases, an opening of the intestine is made over the abdomen called ostomy (ileostomy or colostomy). This is temporary and is closed after the improvement in patients' condition and chemotherapy (if required).
Total colectomy or subtotal colectomy
Sometimes, the whole colon is removed. Done in patients whose part of the colon not involved with cancer has a problem such as multiple polyps, inflammatory bowel disease or dilatation because of intestinal obstruction.
There are two ways to do a colectomy:
Open surgery
A single long incision is made over the abdomen to do the surgery.
Laparoscopic or robotic
The laparoscopic approach uses minimally invasive techniques to do the same surgery with tiny incisions. This entails the insertion of special long thin surgical tools through these small holes. This results in faster recovery and reduced pain compared to conventional open surgery. This requires expertise. Make sure your surgeon is skilled and has done many of these operations.
Robotic surgery combines the skill and expertise of a surgeon with the vision, precision, and flexibility of robotic technology. The robotic system features a 3D high-definition camera system for clear and enhanced vision with depth perception. It comprises a surgical console, where the surgeon sits, and robotic arms equipped with surgical instruments. The tiny wristed instruments can bend and rotate in ways the human hand cannot, allowing the surgeon to operate in tight spaces.
During robotic surgery, the surgeon makes minor cuts in the abdomen and inserts special tubes called ports. The robotic arms are connected to these ports, and the instruments mounted on these robotic arms go through the ports to do the surgery. A slender camera is also inserted through one port to show the surgeon a clear view of the inside. The surgeon controls the robotic arms from a console nearby, and an assistant helps by changing the instruments and aiding as needed.
Cancer will sometimes block the colon, a condition called intestinal obstruction. In such cases, a stent may be placed to relieve the obstruction, improve the condition of the patient and then do the surgery. If the stent can't be placed or is not available, direct surgery is done. In such cases, usually, the ends of intestine are not reconnected but brought out as stoma. The ends of the intestine are reconnected later in a second operation when the health of the patient improves.
Treatment of advanced colon cancer
Curative surgery for advanced colon cancer
Some stage IV cancers have spread limited to few spots of cancer in the lung, liver and peritoneum. If both colon and all these spots can be safely removed, then surgery can attempt to cure the disease.
Liver resection for colon cancer
It is a surgical procedure to remove cancer containing part of the liver, also called hepatectomy or metastasectomy.
Lung resection for colon cancer
Pulmonary (lung) resection is a surgical procedure to remove the part of the lung, which has cancer.
Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC) for colon cancer
Cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (HIPEC) treats colorectal cancers that have limited spread to the abdominal cavity (peritoneum). During cytoreductive surgery, all visible tumours are surgically removed, which only leaves microscopic cancer cells. Cytoreductive surgery is followed by HIPEC, which aims to destroy the remaining microscopic cancer cells. In HIPEC, concentrated and heated chemotherapy solution is delivered directly into the abdominal cavity which kills those cells.
This approach helps the patients live longer and provides them with a chance to be free of cancer over the long term. We prefer to give neoadjuvant treatment before surgery in these patients.
Liver-directed therapy - curative
Besides surgical resection, tumours which have spread to few spots in the liver or lung are sometimes treated by embolization or ablation.
Embolization for colorectal cancer liver metastasis
Embolization means blocking the blood supply of the tumour. A catheter is passed into the vessel supplying the tumour and is blocked with small particles and other agents. Chemotherapeutic agents and radioactive beads can also be delivered directly into the tumour during this, called chemoembolization or radioembolization.
Ablation for colorectal cancer metastasis
Ablation uses extreme heat, cold or chemical to kill the tumour cells. This is best for small tumours which are less than 2 cm. Radiofrequency ablation (RFA) uses high-frequency radio waves to generate heat and kill the tumour. A probe is inserted into the tumour guided by ultrasound or CT scan. Microwave ablation uses microwaves to generate heat and kill the tumour. Cryoablation or cryotherapy kills the tumour by freezing it with a metal probe. Percutaneous ethanol injection (PEI) can also be given into the tumour killing the cells.
Palliative surgery for advanced colon cancer
Ostomy (ileostomy or colostomy) is an operation to make an opening in the intestine and bring it out by creating a hole in the abdomen's wall. It excretes stool into a bag that fits securely over the opening. The surgeon does an ostomy when the tumour has grown too big and causes intestinal obstruction (blockage) while the patient is unfit to undergo major surgery to remove the tumour or cancer has spread to other parts of the body.
Chemotherapy for colon cancer
Chemotherapy uses drugs to destroy cancer cells. Several drugs are combined together and given in a specific order on specific days as cycles.
Adjuvant chemo: In patients with localized colon cancer, chemotherapy is usually given after surgery to kill the cells which could remain. The decision to give chemotherapy depends on the surgical stage. It is usually administered if cancer has spread to lymph nodes or penetrated into outer layers of the intestine. In this way, chemotherapy helps reduce the risk of cancer recurrence and death from cancer.
Neoadjuvant chemo: If the tumour has excessively grown, then chemotherapy is administered before surgery. It will shrink cancer and produce a better result from an operation later.
Palliative chemo: In metastatic cancers chemotherapy prolongs survival and improves the quality of life.
Targeted therapy for colon cancer
Substances which identify and attack cancer cells without harming normal cells.
Monoclonal antibodies
Made from a single type of immune system cells.
Vascular endothelial growth factor (VEGF) inhibitor: VEGF causes tumours to grow and new vessels to form. VEGF inhibitors block this pathway.
Epidermal growth factor receptor (EGFR) inhibitors: EGFR is proteins on the cell surface of cancer cells which help in their growth. EGFR inhibitors block the protein and stop the cancer cells from growing.
Kinase inhibitors: Substances that block a type of enzyme called kinase. Human cells have many different kinases, and they help control important functions, such as cell signaling, metabolism, division, and survival.
Immunotherapy for colon cancer
It uses the patient's immune system to fight cancer. Immune checkpoint inhibitor therapy is a type of immunotherapy.
Radiation therapy
Radiation therapy uses high energy X-rays to destroy cancer cells. It is not usually used for colon cancer. It can occasionally be used in select cases of colon cancer.
Prognosis of colon cancer
Survival rates of colon cancer
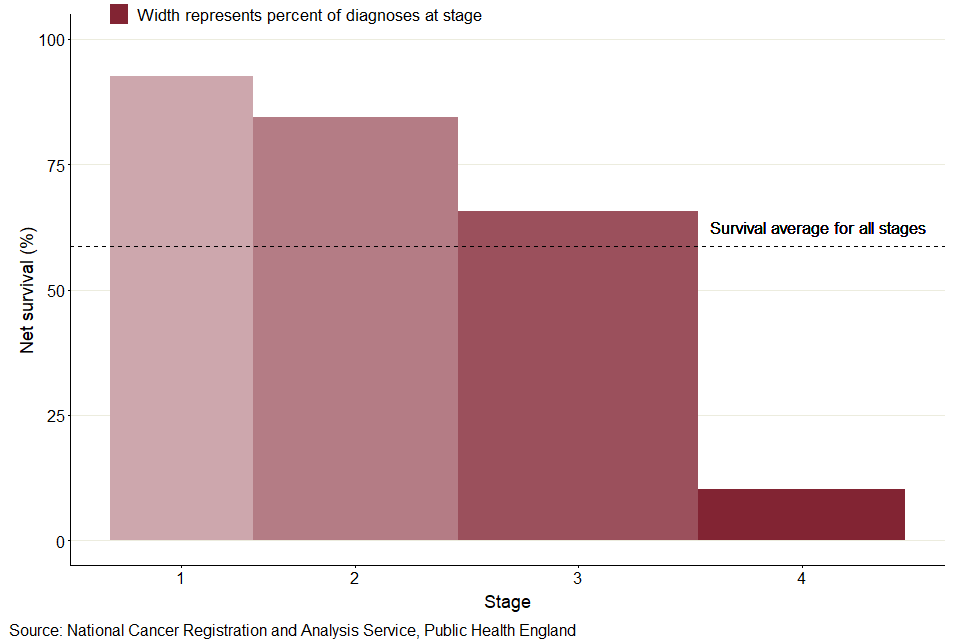
It is often measured as 5-year survival. It is the percentage of people with the same type and stage of cancer who are alive 5 years after diagnosis. These estimates are generated from many patients. After treatment for stage 1 colon cancer, the 5-year survival is slightly over 90%. For stage 2 it is roughly 60-90%. The 5-year survival for stage III colon cancer varies from 45 to 90% and for stage 4, the 5-year survival is approximately 15%.
Screening for colon cancer
If we can find diseases earlier, we can treat them better. Screening is a proactive approach to detect cancer in apparently healthy individuals who have no symptoms.
It takes 10-15 years for an abnormal cell to develop into colon cancer. We can even remove them at the stage of a polyp and prevent cancer from occurring. However, not everyone needs screening. Screening is done in individuals at high risk of developing colon cancer.
Screening tests for colorectal cancer include faecal immunochemical test or guaiac-based faecal occult blood test on stool, colonoscopy, CT colonography and sigmoidoscopy.
Who should be screened for colorectal cancer?
- If your age is over 45 years.
- If you have a family history of colorectal cancer or polyps
- If you have a personal history of colorectal cancer or polyps
- If you are suffering from long-standing inflammatory bowel disease (ulcerative colitis or Crohn's disease)
- If you have a family history of a hereditary colorectal cancer syndrome such as familial adenomatous polyposis (FAP) or Lynch syndrome (also known as hereditary non-polyposis colon cancer or HNPCC)
- If you have a history of radiation to the abdomen (belly) or pelvic area to treat a prior cancer
How to lower your risk of colon cancer?
We can categorise the risk factors for colorectal cancer into modifiable and non-modifiable. Age and genetic factors are non-modifiable and we can't do anything about it. However, we can decrease the risk by avoiding the risk factors which we can control.
We can lower our risk by taking the following steps:
- Maintain a healthy weight
- Regular physical activity and exercise
- Eat a healthy diet especially rich in fibre fruits, vegetables and whole grains while avoiding processed food
- Avoid smoking and tobacco
- Limit alcohol
Detect Early, Treat Right, Save Lives!

About Author
Dr. Nikhil Agrawal
MS, MCh
Dr. Nikhil Agrawal is a leading GI-HPB Surgical Oncologist with 20+ years of experience in complex cancers of the esophagus, stomach, colon, rectum, liver, pancreas, gallbladder, and bile ducts. He leads the GI-HPB Oncology Program at Apollo Hospitals, Delhi and Gurugram, with expertise in advanced robotic and laparoscopic cancer surgery.
His practice focuses on evidence-based, multidisciplinary care with an emphasis on individualized treatment and long-term outcomes.
He trained at BHU, SGPGI Lucknow, AIIMS New Delhi, and SNUBH, South Korea, and is a robotic surgery proctor who trains surgeons in advanced GI-HPB cancer surgery. He is also regularly invited as faculty at national and international scientific meetings.
This website helps patients and families understand GI and HPB diseases and cancers, treatment options, and what to expect during recovery and long-term care.