Bile duct cyst
Choledochal cyst
Cystic dilatation of the bile duct


The bile duct
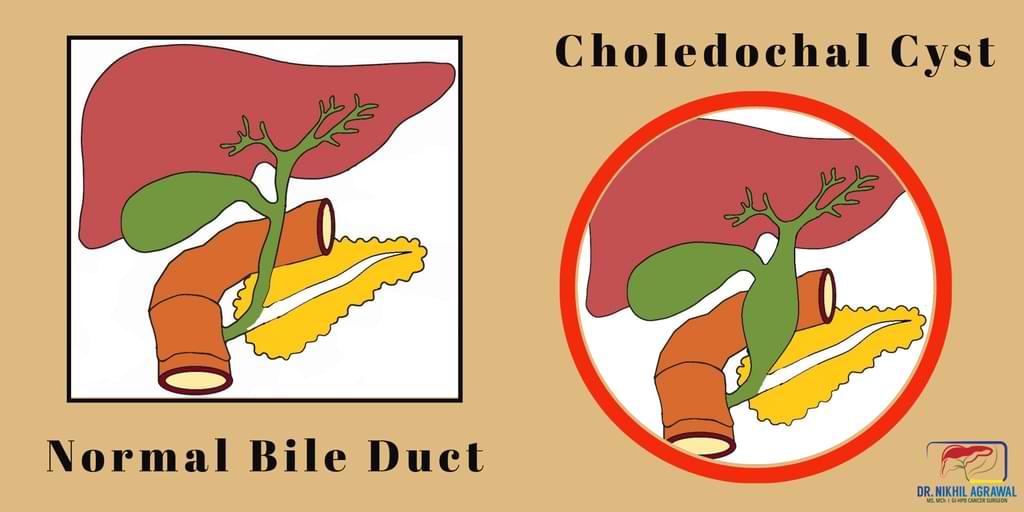
Bile is a fluid made by the liver to aid digestion of fats in the intestine. The bile duct is a network of thin tubes. It collects bile from the liver and brings it to the intestine. The bile duct is a tree-like structure with multiple branches in the liver. These branches combine to form the right and left duct (hepatic duct) collecting bile from the right and left lobe of the liver. These two (right and left hepatic ducts) then join; the joint called hilum or confluence and becomes the common hepatic duct (CHD). The gallbladder joins CHD through the cystic duct and forms the common bile duct (CBD). The common bile duct then continues downstream, the pancreatic duct joins it and the common channel opens into the intestine (in the intestine's part called the duodenum).
The choledochal cyst
A cyst is a fluid-filled, sac-like structure with a thin membranous wall. A choledochal cyst is a cyst of the bile duct. Choledochal cyst is also called bile duct cyst.
Types and locations of choledochal cysts
The choledochal cyst can affect the bile duct inside the liver (intrahepatic), outside the liver (extrahepatic) or the whole bile duct. It can form as an outpouching (diverticulum-like) from the duct or it can be a limited dilatation (expansion; distension) of the part or whole of the duct.
Based on these, there are five types of choledochal cysts:
- Type 1: It is the most common type. It is a cyst of the extrahepatic bile duct.
- Type 2: It is an outpouching from the bile duct.
- Type 3: It is a cyst of the bile duct inside the wall of the duodenum where the bile duct ends.
- Type 4: Multiple cysts of the extrahepatic bile duct or both intrahepatic and extrahepatic bile duct.
- Type 5 or Caroli's disease: Cystic dilatation of intrahepatic bile duct.
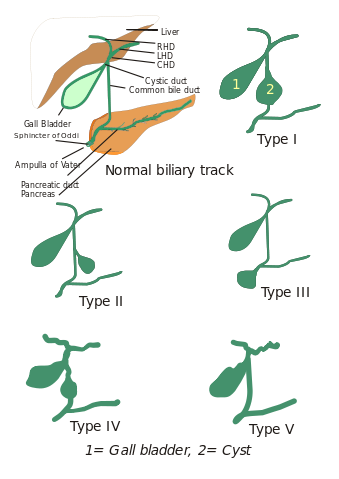
I, Drriad, CC BY-SA 3.0, via Wikimedia Commons
Causes of choledochal cyst
Choledochal cysts are rare, and the cause is largely unknown. The abnormality is congenital (present from birth). Researchers believe choledochal cysts form when there is an abnormality at the joint of the bile duct and pancreatic duct.
Signs and symptoms of choledochal cyst
Although the abnormality in the bile duct is present since birth, symptoms may appear in childhood or later.
The following symptoms may occur:
- Abdominal mass
- Pain in the right upper abdomen
- Jaundice (yellowing of eyes, urine and skin
- Nausea and vomiting
- Recurrent fever
Sometimes these do not cause symptoms and are picked up on tests done for some other illness or on a routine check-up. Some of these patients may present later in their life with complications related to bile duct cysts.
Complications of choledochal cyst
If left untreated for long, there is an increased risk of developing cancer of the bile duct and gallbladder cancer.
The choledochal cyst or the stone in it. may block the flow of bile causing jaundice. If it is not treated, permanent damage may occur to the liver. Sometimes they may cause pancreatitis (inflammation of the pancreas). Some Type 4 and 5 choledochal cyst can cause the formation of stones in the liver, atrophy (shrinkage) of part of the liver or abscess formation in the liver.
Diagnosis of choledochal cyst
Diagnosis means identifying a disease.
Following tests will help us make the diagnosis of choledochal cyst.
Physical history and examination
Understanding symptoms and checking for signs by a physician are basics of arriving at a diagnosis.
Blood tests
Complete blood count measures the distinct cells in the blood. Liver and kidney function tests assess the function of these organs. Some of the patients will have an abnormal liver function test.
Ultrasound (USG)
This is a basic test to see the liver and bile ducts. An ultrasound scan uses high-frequency sound waves to create an image of the inside of the body.
Magnetic resonance imaging (MRI) and magnetic resonance cholangiopancreatography (MRCP)
MRI uses strong magnetic fields, radio waves and computer to generate images of inside organs. This imaging modality gives a detailed view of the bile duct and cancer.
Treatment of choledochal cyst
The best way to treat choledochal cyst is to surgically remove it. Some of the patients who present with jaundice, cholangitis or pancreatitis, may require treatment of these conditions first. Surgery is done once the patient has recovered.
Surgery for choledochal cyst
The complete excision of the bile duct cyst should be done (from the confluence above to the junction with the pancreatic duct below). Following excision, the pathway of the flow of bile is restored by joining the intestine to the remnant part of the bile duct. This is called hepaticojejunostomy. If a part of the liver is damaged, it is also removed. The surgical procedure is called hepatectomy or liver resection.
There are two ways to do the operations for bile duct cysts;
- Open, and
- Laparoscopic or Robotic
In open surgery, a single long incision is made over the abdomen to do the surgery.
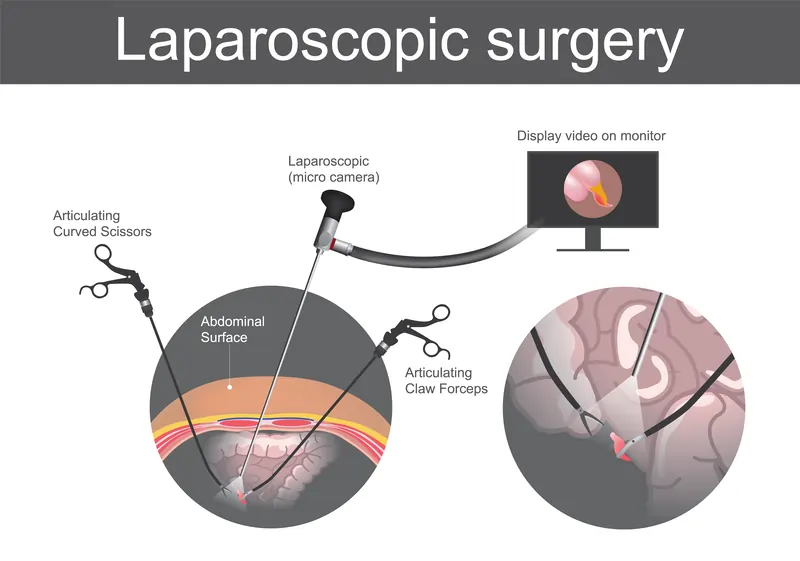
Laparoscopic surgery for choledochal cyst
The laparoscopic approach uses minimally invasive techniques to do the same surgery with tiny incisions. This entails the insertion of special long thin surgical tools through these small holes. This results in faster recovery and reduced pain compared to conventional open surgery. This requires expertise.
Robotic surgery for choledochal cyst
Robotic surgery combines the skill and expertise of a surgeon with the vision, precision, and flexibility of robotic technology. The robotic system features a 3D high-definition camera system for clear and enhanced vision with depth perception. It comprises a surgical console, where the surgeon sits, and robotic arms equipped with surgical instruments. The tiny wristed instruments can bend and rotate in ways the human hand cannot, allowing the surgeon to operate in tight spaces.
During robotic surgery, the surgeon makes minor cuts in the abdomen and inserts special tubes called ports. The robotic arms are connected to these ports, and the instruments mounted on these robotic arms go through the ports to do the surgery. A slender camera is also inserted through one port to show the surgeon a clear view of the inside. The surgeon controls the robotic arms from a console nearby, and an assistant helps by changing the instruments and aiding as needed.
Long-term complications after surgery
Future complications include cholangitis (infection of the bile duct) and a 2% risk of malignancy, which may develop in any part of the biliary tree.
Detect Early, Treat Right, Save Lives!

About Author
Dr. Nikhil Agrawal
MS, MCh
Dr. Nikhil Agrawal is a leading GI-HPB Surgical Oncologist with 20+ years of experience in complex cancers of the esophagus, stomach, colon, rectum, liver, pancreas, gallbladder, and bile ducts. He leads the GI-HPB Oncology Program at Apollo Hospitals, Delhi and Gurugram, with expertise in advanced robotic and laparoscopic cancer surgery.
His practice focuses on evidence-based, multidisciplinary care with an emphasis on individualized treatment and long-term outcomes.
He trained at BHU, SGPGI Lucknow, AIIMS New Delhi, and SNUBH, South Korea, and is a robotic surgery proctor who trains surgeons in advanced GI-HPB cancer surgery. He is also regularly invited as faculty at national and international scientific meetings.
This website helps patients and families understand GI and HPB diseases and cancers, treatment options, and what to expect during recovery and long-term care.